An aneurysm is a bulge on the wall of an artery. This occurs because of a weak spot in the artery wall, which could potentially rupture.
Brain aneurysms are in fact quite common and most aneurysms do not cause any symptoms or problems. However, a small proportion of aneurysms can rupture and lead to bleeding in the brain – a type of stroke called a subarachnoid haemorrhage.
This is a medical emergency that requires immediate treatment. In this article, you can learn about the symptoms, diagnosis, and treatment options for aneurysm.
Click the headings below to jump to a specific section.
What is an aneurysm?
Cerebral aneurysm is a bulge or ballooning on the wall of a brain artery. It is a common condition caused by a weakness in the artery wall, affecting approximately 3-5% of the population (1).
In the vast majority, aneurysms do not cause any symptoms or ill-effects as they are intact and do not rupture. Many people do not know they have one until it is detected in another test or routine screening. It is also quite common for people to have multiple small aneurysms.

However, in a small proportion of individuals, the aneurysms rupture and cause a dangerous bleeding in the brain (a type of stroke called subarachnoid haemorrhage). Symptoms of a ruptured aneurysm include a sudden, severe headache, nausea and vomiting, loss of consciousness or seizures. Seek emergency medical help or call 000 if you see someone with these symptoms.
Causes & risk factors
Many aneurysms form spontaneously and do not have a clear cause. However, they are more common in certain populations, and several risk factors have been identified. These risk factors contribute towards the formation and rupture of aneurysms (2):
- Hypertension (high blood pressure). This means there is increased pressure against the artery walls.
- Older women. Researchers believe that oestrogen helps to prevent aneurysm, so risk increases when oestrogen levels drop after menopause.
- Age. Aneurysm is more common in people aged 45-65.
- Family history. In some cases, a family history of aneurysm can increase risk.
- Smoking or high alcohol consumption. These are well-established risk factors, however you can reduce your risk level by quitting smoking and reducing your alcohol intake.
It is quite rare for an aneurysm to rupture – only about 0.95% of aneurysms rupture each year (1). Rupture is more likely if the aneurysm is particularly large or if it is located on the Posterior or Anterior Communicating Artery (1).
Symptoms
An unruptured aneurysm usually does not cause any symptoms, particularly if it is small. When they do cause symptoms, these symptoms are often vague and non-specific (which means they can be caused by many other conditions as well), such as headache or dizziness (3). If you have a persistent or unusual headache it’s always a good idea to see a doctor.
However, larger ones might press on your nerves, which could cause:
- Pain above and behind one eye
- A dilated pupil
- A change in vision or double vision
Unfortunately, symptoms often only appear after the aneurysm ruptures. The rupture causes bleeding in the brain called a subarachnoid haemorrhage, which is a type of stroke. The most significant symptom is a sudden, abrupt, severe headache, especially during exertion (4). It is often described as the “worst headache ever experienced” or a “thunderclap headache” when the pain is so abrupt that the maximum intensity of the headache occurs instantly.
Other symptoms could include:
- Nausea and vomiting
- Neck stiffness
- Blurred or double vision
- Light sensitivity
- Seizures
- A drooping eyelid
- Loss of consciousness
- Confusion

Diagnosis
If an aneurysm is unruptured it can remain undetected for a long time. It is often only found by chance – for example, if you are getting a brain scan for an unrelated condition. Some of the tests that can detect an aneurysm include:
- Computed tomography scan (CT or CAT scan) with angiography
- Magnetic resonance imaging (MRI) with angiography
Many cases are not discovered until the aneurysm ruptures.

Aneurysm treatment
There are several options for treating both ruptured and unruptured aneurysms. These include (5):
- Clipping. A surgical procedure in which a neurosurgeon removes a piece of your skull to locate the blood vessel, and places a tiny metal clip on the neck of the aneurysm. This stops blood from flowing into the aneurysm.
- Endovascular procedures. These are less invasive. The surgeon inserts a catheter into an artery in the leg and passes it through the natural blood vessels system in the body to the aneurysm. They then use a device to seal off the aneurysm.
- Coiling. Coiling involves inserting platinum coils into the aneurysm, which cause the blood to clot and seal off the aneurysm.
- Stents. A mesh stent is sometimes used alongside coiling. A stent is a metal, chicken-wire like device that holds the coil in place. This is necessary if the opening of the aneurysm is very wide or an unusual shape.
- Flow diversion. A flow diversion device is similar to a stent but it is made of a much tighter mesh. It’s a cylindrical tube made of braided wires which is inserted into the blood vessel next to the aneurysm opening. This allows blood to bypass the opening and flow through the vessel normally.

A) Coiling, B) Clipping, C) Coil with stent, D) Flow diversion.
Image source: M N Ngoepe et al, 2018, Thrombosis in Cerebral Aneurysms and the Computational Modeling Thereof: A Review. DOI: 10.3389/fphys.2018.00306
The type of treatment will depend on the size and location of the aneurysm, your ability to undergo a procedure, and other factors. This is because these procedures are risky and could cause a bleed in the brain or block off blood flow. If the aneurysm has ruptured, it should ideally be secured as soon as possible, within the first few days of rupture (5).
Endovascular devices (coils, stents, diversion) are generally safer because they are less invasive, but they carry a higher risk of the aneurysm re-opening in the future. Surgical clipping is a riskier procedure, but it is slightly more effective in the long term.
If the aneurysm is unruptured, your doctor might decide it is best to focus on risk factors management and observation. This is because the risk of rupture may be so low that it does not need to be treated by clipping and endovascular devices. Risk factors management includes things like quitting smoking and lowering your blood pressure. They will only recommend treatment if it is safe and necessary (i.e. if it has a high risk of rupturing).
Summary: What factors are considered when making a decision about aneurysm treatment?
- Rupture status
- Symptomatic vs asymptomatic
- Family history & genetics
- Associated risk factors: hypertension, smoking, alcohol, drug use
- Size of aneurysm
- Aneurysm location: anterior vs posterior circulation, anterior or posterior communicating segment, extradural vs intradural
- High risk aneurysm characteristics:
- Change of size or morphology over time
- New neurologic or cranial nerve symptoms
- Irregularities and daughter lobes
- Prior subarachnoid haemorrhage
- Patient’s age, functional status, and comorbidities
- Life expectancy
- Anatomy of blood vessels
- Predicted risk of surgical or endovascular treatment
Source: G Toth & R Cerejo, 2018, Intracranial aneurysms: Review of current science and management [Table 7].
Prevention
In many cases, aneurysms develop naturally. However, there are a few risk factors that you can control to minimise the aneurysm developing, growing and causing problems.
- Don’t smoke or use recreational drugs. You can talk to your healthcare provider about strategies or a treatment plan to help you quit.
- Avoid heavy alcohol consumption. Adults should drink no more than 4 standard drinks per day, and no more than 10 standard drinks in a week.
- Eat a healthy diet and exercise. A well-balanced diet and exercise can help manage your blood pressure. There are options available for all lifestyles – it doesn’t have to involve an expensive meal plan or daily gym sessions! Your healthcare provider can help you make appropriate choices.
- Control your blood pressure if you have high blood pressure. Sometimes, medication is necessary to manage blood pressure.
If you have a family history of cerebrovascular disease (including stroke, AVM, aneurysm, etc), managing these risk factors could reduce your likelihood to develop an aneurysm.
In general, maintaining a healthy lifestyle is a good rule of thumb to prevent many neurological conditions. However, people who follow all these guidelines can still develop brain diseases. It’s important to remember that developing an aneurysm or any other disease is not your fault, and there are treatment options and support services available.
Prognosis
The outlook after rupture of a cerebral aneurysm depends on the size and location of the aneurysm, the person’s age, general health, and neurological condition after haemorrhage. On average only about 0.25% of aneurysms are estimated to end in rupture (5). However, if they do rupture, there is a serious risk of death or disability after the subarachnoid haemorrhage (SAH).
The graph below shows the discharge outcomes of people who were hospitalised for SAH, split across different age groups. Some of these people were treated with a clipping procedure and others were treated with coiling (or another endovascular treatment).
Discharge outcomes for SAH patients, 2005-2009
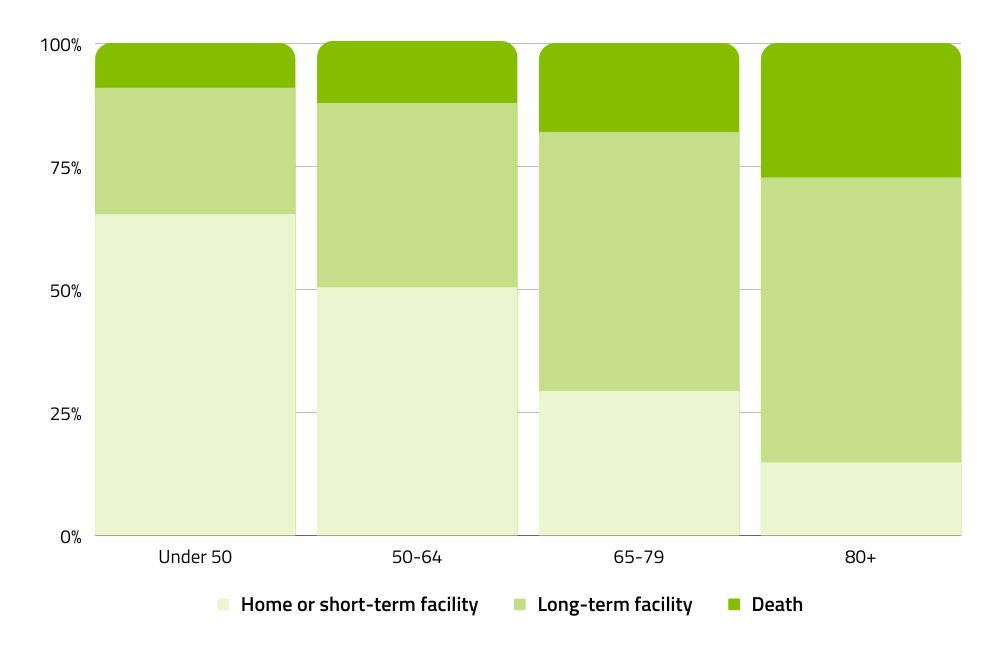
*Exact percentages of home/short-term facilities, long-term facilities, and death are as follows for each age group: <50 = 65.2, 25.7, 9.1; 50-64 = 50.0, 37.6, 12.6; 65-79 = 29.3, 52.6, 18.1; 80+ = 14.8, 57.9, 27.3.
Source: W Brinjikji et al, 2013, Age-Related Trends in the Treatment and Outcomes of Ruptured Cerebral Aneurysms: A Study of the Nationwide Inpatient Sample 2001–2009 [Figure 2].
It is important to note that this study only looked at patients who already had a ruptured aneurysm. It is possible to treat an aneurysm before it ruptures if it is diagnosed early enough.
Other studies investigating mortality and disability after SAH have found that (7):
- 15-20% of patients die before reaching the hospital
- A further 20-25% die within 48 hours
- The total 30-day mortality rate after SAH can be as high as 50%
- Approximately 30% of survivors become dependent on others due to disability
The most common impairments after haemorrhage include cognitive and neurological impairments in (7):
- Attention
- Mental flexibility
- Visual working memory
- Verbal fluency
- Response inhibition
- Visual constructive ability
- Visual memory
These changes can limit a person’s ability to complete day-to-day tasks and return to work. Some people are able to recover cognitive function over time through rehabilitation, but in other cases disability can be permanent.
Thankfully there have been many advances in treatment over the years that have improved outcomes for aneurysm and haemorrhage patients. Mortality rates have declined 0.9% per year over the past 2 decades, and we hope to see this trend continue (7).
Further information & resources
If you would like to learn more about aneurysm, you can explore the following articles, resources, and support organisations:
- Read the latest Australian research papers on aneurysm via the National Library of Medicine >
- Surviving an aneurysm – read Andy’s story about her experience with aneurysm.
- Brain Injury Australia – BIA provides resources and support services for people living with brain injury (including aneurysm/SAH).
- Brain Aneurysm Foundation USA – an American organisation whose mission is to promote early detection of brain aneurysms by providing knowledge and raising awareness of the signs, symptoms and risk factors.
- British Brain and Spine Foundation – a UK organisation that raises awareness for many different brain diseases, disorders & injuries. They have some downloadable resources about aneurysm & SAH.
References:
- N Chalouhi et al, 2013, Review of Cerebral Aneurysm Formation, Growth, and Rupture. DOI: 10.1161/STROKEAHA.113.002390
- S E Francis et al, 2013, A combination of genetic, molecular and haemodynamic risk factors contributes to the formation, enlargement and rupture of brain aneurysms. DOI: 10.1016/j.jocn.2012.12.003
- A Cianfoni et al, 2013, Clinical presentation of cerebral aneurysms. DOI: 10.1016/j.ejrad.2012.11.019
- JJ Perry et al, 2013, Clinical Decision Rules to Rule Out Subarachnoid Hemorrhage for Acute Headache. DOI: 10.1001/jama.2013.278018
- G Toth & R Cerejo, 2018, Intracranial aneurysms: Review of current science and management. DOI: 10.1177/1358863X18754693
- W Brinjikji et al, 2013, Age-Related Trends in the Treatment and Outcomes of Ruptured Cerebral Aneurysms: A Study of the Nationwide Inpatient Sample 2001–2009. DOI: 10.3174/ajnr.A3321
- S Dey et al, 2018, Neurological, neuropsychological, and functional outcome after good grade aneurysmal subarachnoid hemorrhage. DOI: 10.4103/0028-3886.246243

DISCLAIMER: The information provided is designed to support, not replace, the relationship that exists between a patient / site visitor and his / her existing health care professionals.